
Impingement of the shoulder
Subacromial Impingement is a common cause of a painful shoulder. It has also been referred to as tendonitis or bursitis of the shoulder. More recently a term of Subacromial Pain Syndrome has been adopted.
What happens?
The space between the rotator cuff tendons and the under surface of the acromion, which is referred to as the subacromial space. This contains a bursa which helps free movement of the arm and its tendons. When the arm is away from the body this space is reduced. Normally this doesn’t cause a problem.
But symptoms can either occur spontaneously, or after a minor injury or overuse of the shoulder.
.

Typical pain is in the outer part of the shoulder, this can be felt in the upper arm and as far down as the elbow. Activities where the arm is used away from the side of the body or the arm is rotated are painful. Patients often have difficulty lying on the affected side.
Typical features
- Pain outer shoulder and upper arm
- Worse on reaching above the shoulder
- Worse on rotation of the arm
- Night pain

Assessment
Clinical assessment is based on the history and examination of the patient. It is important to rule out any contribution from other areas such as the neck. If there is a weakness in the arm then a rotator cuff tear is suspected and this can be investigated by an Ultrasound or MRI scan.
Treatment
Initial treatment is usually non operative with physiotherapy initially and a subacromial steroid injection. This will resolve the problems in the majority of patients. The aim of non operative treatment is to improve function and pain. Correctable problems (with rehab) which can occur in impingement are:
- Tight posterior capsule
- Poor scapula control
- Altered scapulohumeral rhythm
Physiotherapy can take 6-12 weeks to see any benefits, The British and Elbow and Shoulder Society recommend several exercises such as Wall sides, push ups against a wall and shoulder rotation exercises. Up to 2 steroid injections can be used to help reduce pain. There is no current evidence to say that image guided injections are superior to injections done in the outpatient clinic.
If this fails then one must consider the following;
- Is the diagnosis correct? Other causes: neck etc
- Is there a rotator cuff tear?
- Is surgery required?
Surgery
The role of surgery is controversial in subacromial pain syndrome and is generally now only considered as a last resort.
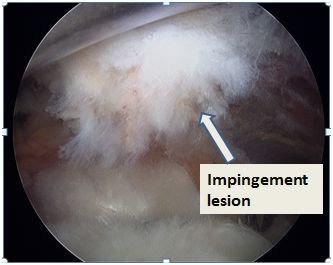
Surgery is performed to increase the subacromial space and to remove inflamed tissue, arthroscopic (key hole) surgery allows the rest of the shoulder and rotator cuff to be inspected. This is done by removing about 5mm of bone from the underside of the acromion and releasing the ligament which forms the arch. Read more
The benefits of surgery include;
- Increased space above the rotator cuff
- Removing bone and releasing ligament
- Removing inflamed tissue
- Arthroscopic (key hole) surgery
Rehabilitation
After surgery the arm is in a sling for comfort, but pendular and active assisted exercises are started straight away under the careful guidance of a physiotherapist
Andy Brooksbank

CONSULTING HOURS
CONTACT DETAILS
CONDITIONS
Treatment journey

APPOINTMENTS
Make a consultantion appointment wiith Mr Andrew Brooksbank at BMI Ross Hall Glasgow.

FAQ’s
Frequently asked questions about appointments, treatment, recovery and insurance/payments.
