
1st time dislocation of the shoulder
First time dislocation of shoulder
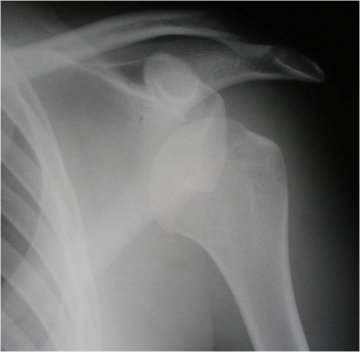
The majority of dislocations of the shoulder are traumatic and the humeral head (ball) dislocates anteriorly (comes out of the front of the socket). The initial treatment of this injury is to have the shoulder put back in joint. This should be carried out in the local Accident and Emergency department usually under sedation. The arm is then immobilised in a sling.
What is the risk of this happening again?
Once a shoulder has dislocated it is more likely for this to happen again. The relative risk of this is greater the younger the individual is and the more at risk activities they do. Men are at higher risk than females and males under 20 have about a 70-80% chance of redislocating their shoulder within 2 years of the initial event. Men under 30 have about a 50-60% chance of redislocation. At risk activities would include most sports where contact / falls are common.
iincreased risk with:
- male
- contact sports
- young age
- bone loss on the humerus or glenoid
What is injured?
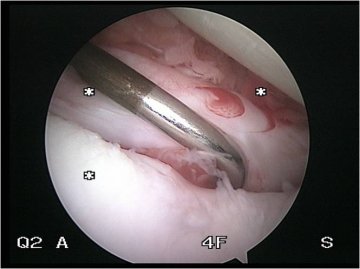
At the time of the injury there are a number of structures that can be injured. The most common pattern of injury is that the lining of the socket which acts to deepen it is ripped off (torn labrum also known as a bankart lesion). The labrum provides an attachment for the ligaments at the front of the shoulder (glenohumeral ligaments). These ligaments can be stretched at the initial dislocation but it tends to occur with further dislocation. With higher impact injuries there can also be injuries to the bone of the socket or of the humeral head (Hill Sachs lesion). The Hill Sachs lesion does not usually cause a problem, but a bony injury to the socket can produce recurrent dislocations.
The Xray shows a dislocated shoulder and the picture shows a torn labrum
What is the treatment?
Traditional treatment is to rest the shoulder in a sling for a period of 2-3 weeks, followed by a period of physiotherapy rehabilitation.
However research has been performed to compare the results of early operation with arthroscopic stabilisation (keyhole surgery). This brought down the risk of redislocation to 15% in the published results. But this does not prevent the shoulder dislocating if a second significant injury occurs.
What happens at surgery?
Arthroscopy is used to repair the torn labrum back to the edge of the glenoid (socket). This acts to deepen the socket and retension the ligaments. Suture anchors are inserted into the bone which allows us to suture the soft tissues down. For this to be successful the torn labrum needs to heal back to the edge of the socket. The shoulder is rested in a sling for a period of usually 4 weeks. Read more
Will I need physiotherapy after?
Yes.
This is an important part of the treatment and is vital to the overall outcome. Rehabilitation can take 3-4 months and the return to sport is dependent on the type and level of activity.
Andrew Brooksbank

CONSULTING HOURS
CONTACT DETAILS
CONDITIONS
Treatment journey

APPOINTMENTS
Make a consultantion appointment wiith Mr Andrew Brooksbank at BMI Ross Hall Glasgow.

FAQ’s
Frequently asked questions about appointments, treatment, recovery and insurance/payments.
